

The Affordable Care Act A.K.A. The Health Security Act 2.0
Obamacare is the offspring of Clintoncare, not the Heritage Foundation


If you were paying attention to the Affordable Care Act (ACA) debate of 2009-2010, or if you are interested in health policy generally, you made have heard someone say, “Obamacare was a Heritage Foundation idea,” perhaps even from former President Obama himself. The idea goes that the Heritage Foundation, a right-wing think tank, was an early advocate of marketplaces where Americans could shop for competing plans, as well as use refundable tax credits to help pay their premiums. Because the ACA marketplace (AKA Obamacare) uses a marketplace and refundable tax credits, and because the ACA came after this Heritage Foundation plan, then Obamacare is fundamentally a Heritage Foundation plan. Considering the continued opposition from right-wing politicians and the Heritage Foundation itself, I have always thought this claim was disingenuous. Furthermore, I think a deeper explanation on the differences between the ACA and the Heritage Foundation plan will show that the similarities of these plans end at the use of tax credits, and denying this ignores key differences in ideology between conservatives and the center-left on the relationship between government and access to health care.
To understand why I don’t think Obamacare is truly a development from the Heritage Foundation plan, I will review: the policy proposal that the Heritage Foundation plan was a response to, the Heritage Foundation plan itself, how the ACA reformed health coverage, and the failed efforts to modify or repeal the ACA in 2017. In the end, I believe Obamacare is not the ideological offspring of the Heritage Foundation plan, but a tailored version of the plan it responded to; while the ACA repeal efforts more closely resembled the Heritage Foundation plan.
President Clinton’s Health Security Act of 1993
As I have explained in previous posts, Bill Clinton is elected in 1992, defeating President George H.W. Bush. Clinton ran partly on a promise to tackle comprehensive health care reform for the first time since the talks between President Nixon and the Democratic Congress collapsed in the 1970s. Though President Clinton did not endorse the single payer proposals espoused by more progressive members of the Democratic Party, he did target a goal of universal health coverage and affordability through private provision and managed competition, cost containment, and subsidization.
The Health Security Act of 1993 relied on regional health alliances responsible for collecting premiums, while states would ensure premiums and bills are paid. The bill set out a deadline for states to set up their regional health alliances and provide coverage for all residents by January 1, 1998, with the Department of Health and Human Services being authorized to withhold federal funds and set up direction operation of the alliances if a state failed to implement the law. A National Health Board would regulate private insurance companies and would set up a national budget for health expenditures each year. A standard package of benefits would be designed and eventually worker’s premiums would not be taxe exempt for services that exceeded the standard benefits. Most Americans would be covered by these regional health alliances, though employers with 5,000 or more employees could continue to manage their own insurance programs. Self-funded plans would not be subsidized, but they would have to have cover at least the standard benefits and spend at least 80% per capita what the government spent. Though the regional health alliances would be mostly run by managed care organizations, doctors could opt for fee-for-service schedules. However, regional alliances would be permitted to set rates for fee-for-service payment. Additionally, physicians would be permitted to enter collective bargaining arrangements to negotiate against regional health alliances. Health spending would eventually have its growth capped to match CPI.
This bill came with significant responsibilities for the States. States had to ensure that at least one plan was available to all residents in every part of the state. States could add to standard benefits, but these benefits were considered the minimum that could be offered. States would monitor the data from these plans, take over plans that failed to ensure continuous coverage for residents, manage state and federal funds to subsidize residents and businesses to afford enrollment, and would have to require 5% to 25% of total costs to a new long term care program. There was also a lack of clarity on the transition from Medicaid to the regional alliance plans, so some advocates worried that alliance plans may be less comprehensive for the poor than some state Medicaid plans.
Insurance regulations would see many changes as well. Patients that believed they were improperly denied coverage could appeal the decision with a new government agency, the Federal Health Plan Review Board that would connect to the larger judicial system. Insurance could no longer be denied based on pre-existing conditions, and premiums would be community rated where all enrollees would be charged the same rates regardless of health status. Greater coverage for preventative services such as immunizations, mammograms, periodic physicals, and more was included. For simpler services, low copays would be offered; for more complex services, 20% coinsurance was standard. Employers would pay at least 80% of the cost of premiums and would pay between 3.5% to 7.9% of payroll towards health expenses depending on their size and the wage of the employee. A similar set up was created to subsidize American’s purchasing directly on the regional health alliances, and Medicaid enrollees would be transitioned to regional health alliances with coverage subsidized as well. Overall, the expectation was that average premiums would be ~$2,000 for a single person and ~$4,400 for a four person household.
To avoid issues of adverse selection, coverage would be mandatory. Residents that did not sign up could pay premiums twice as high as they would have been charged, premiums can be garnished from wages with interest, and civil fines were authorized. There would be no alternative to plans offered on the regional health alliances aside from similarly designed self-funded employer plans or potential single payer schemes.
There would also be changes to Medicare. A prescription drug benefit would be added to Medicare with the federal government able to negotiate on discounted prices after an evaluation of the value of new drugs was conducted. If drug manufacturers and the government could not agree on a discount, then a drug would not be covered by Medicare. High income Medicare enrollees making more than $100,000 per year would be expected to cover 75% of their current premiums rather than the standard 25%.
This plan would be paid for via cuts to national health expenditures via cost control measures tied to inflation, cuts to subsidies for high income Medicare enrollees, a small addition to the corporate income tax, an increase to the tobacco tax, and federal program savings.
The Alternative of the Heritage Foundation Plan
The Heritage Foundation Plan sprang up as a counter to President Clinton’s Health Security Act. Like many conservative groups, the Heritage Foundation derided the Clinton plan as nothing more than big government enforcing one common choice with the only true alternative as state single payer. They rejected the CPI inflation measures as an anti-market measure that would worsen quality of care, standardization of plans as eliminating patient and physician choice, considered the tobacco tax a penalty on personal choice and the inclusion of the community rating and guaranteed issue of health insurance the ultimate perverse incentive to disincentivize people from taking responsibility for their own health, the non-inclusion of self-funded plans was considered a way to penalize large employers that opted out, and mandated coverage its own form of government tyranny (though they were an early proponent of the individual mandate). The Heritage Foundation was further skeptical of regional health alliances and the National Health Board, considering them new government agencies in all but name. And the involvement of the government in evaluating pharmaceutical advances was thought as nothing more than a way to stifle innovation. In short, they were not fans.
As an alternative, The Heritage Foundation offered a simple plan. No regional health alliances, no National Health Board, no new Medicare programs or long-term care program, no new federal insurance regulations or standard benefit packages, and no mandated coverage or community rating. Instead, Americans would receive a simple flat refundable tax credit that would be paid in advance or monthly to help pay for their health insurance premiums. The value of the tax credit could be targeted to be of similar value to the subsidy for the program Federal employees at 75% of the cost of Federal employee health plans, or for 50% of the total cost of the typical health insurance plan. The tax credit was cited at around $3,000 when it was presented to the George W. Bush Administration. To avoid job lock and prevent rampant subsidization of employer insurance, they proposed this tax credit be available to Americans in place of employer coverage as well. As an alternative to strictly regulated standardized insurance plans, they touted the success of health care sharing ministries and association health plans in providing access to health insurance products in the individual market. There would be no new regulation of health insurance as proposed in the Health Security Act. If Americans wanted more comprehensive health coverage, they could pay for it entirely on their own dime past the tax credit’s amount. In theory, this would hold down health care prices by forcing Americans to feel the sting of purchasing their own plans.
The Years Between and the Affordable Care Act
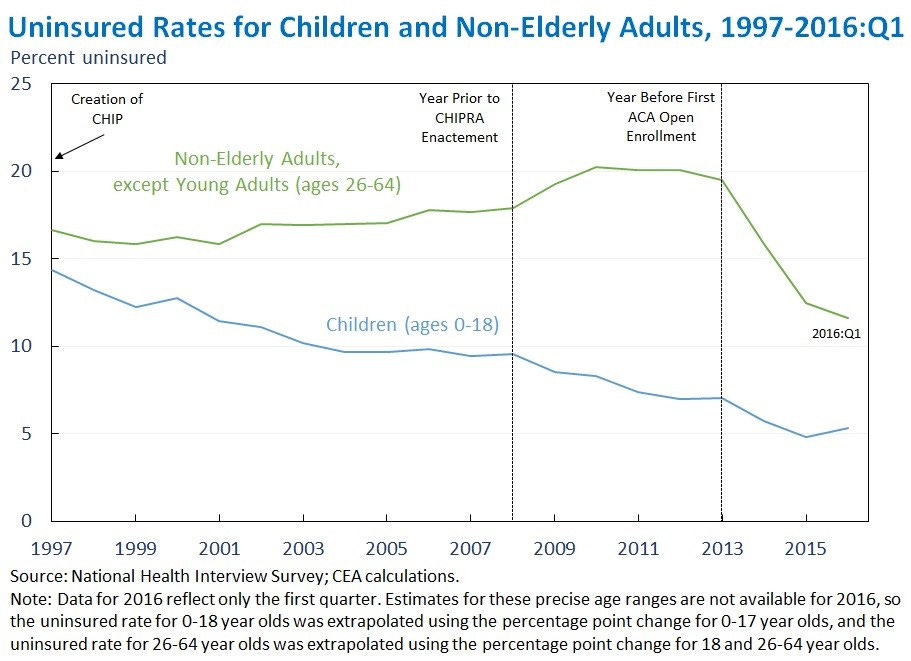
In the end, neither of these plans came to be. The Health Security Act faced its final defeat shortly before the 1994 midterms, and the GOP gained control of Congress for the first time in decades. The new GOP had no interest incomprehensive health care reform, but President Clinton’s position prevented any conservative health care plans from coming to fruition. There was modest bipartisan reform via HIPAA in 1996 that attempted to improve privacy and data protections while ensuring guaranteed issue of insurance for employees with employer coverage. Additionally, the Balanced Budget Act of 1997 created Medicare Choice+ (later Medicare Advantage) to offer a private managed care version of the Medicare program, while also creating the Children’s Health Insurance Program (CHIP) as a block grant for states to cover more children by building on state Medicaid programs, a new separate program, or a mix. Over time, CHIP in combination with other programs reduced the child uninsured rate from nearly 15% in 1997 to around 5% today.
George W. Bush, the son of George H.W. Bush, was elected to succeed President Clinton in a contentious election in 2000. As a part of his agenda, President Bush worked with the GOP Congress and a minority of Democrats to pass the Medicare Modernization Act of 2003. This both created the Medicare Advantage brand we know today, and created a private voluntary prescription drug program to add on to the traditional Medicare program, called Medicare Part D. This program was launched in 2006, but no other major changes to the health care industry occurred until the election of Barack Obama and a staunchly Democratic Congress following the wave elections in 2006 and 2008 to counter GOP successes seen in 1994, 2000, and 2002.

In a repeat of history, President Obama and the Democratic Congress used their newly found trifecta to once again to tackle the issue of comprehensive health care reform. What came of this attempt after over a year of debate was the Affordable Care Act. I have covered this topic in a past post, but here is the gist. In order to guarantee access to health coverage regardless of health status, health insurance on the individual market would not be able to deny coverage for pre-existing conditions (guaranteed issue) just like was done for employer insurance in HIPAA in 1996; and to avoid the complicated underwriting process, ACA market health insurance premiums were to be community rated just like the Health Security Act intended. All plans on the ACA marketplace, small group plans, and employer plans would be required to cover a standardized list of Essential Health Benefits, and self-insured plans would be required to cover preventative care. Individual marketplace plans would range from four tiers: Bronze (60% actuarial value), Silver (70%), Gold (80%), and Platinum (90%). For Americans on the individual market, refundable tax credits were provided, like the Heritage Foundation plan, but these were scaled progressively so that premiums would range by income like the Health Security Act intended. Health insurance plans would be private managed care plans, just like the Health Security Act. Further subsidies were available, Cost-sharing Reductions (CSRs) to lower out of pocket costs for enrollees up to 250% poverty.
Employer plans would require coverage equivalent to at least a bronze plan and employees could only have premiums no more than about 10% of their income. Employers with at least 50 employees would be mandated to offer this minimum quality coverage to 95% of their full-time employees, or face a penalty. Small businesses would be able to earn tax credits to offer employees health plans on a marketplace specific to small businesses, but they were not required to do so. The ACA also included a tax on excessive plans that effectively removed the tax-exempt status of employer insurance premiums similar to the Clinton plan, but this was repealed. Any employee offered a minimum value plan or more by an employer would not be eligible for marketplace subsidies, effectively building a “firewall” between the individual ACA marketplace and the employer marketplace.
To further regulate the market, risk corridors were temporarily set up to stabilize insurance losses and reinsurance would compensate insurance companies in the first few years for high-cost enrollees. Risk-adjustment on and off the ACA market would permanently work to have insurance companies with disproportionately healthy enrollees compensate insurers with a sicker population. And insurance would have to spend a certain percentage of their expenses on medical care or reimburse enrollees.
To prevent adverse selection, the ACA once again relied on a penalty for Americans forgoing purchasing health insurance, the individual mandate. Americans on the individual market would shop for plans during an open enrollment period, and Americans that neglected to purchase plans would have to wait until next year or purchase less well-regulated short-term plans.
These plans would be sold on either a federal facilitated marketplace (FFM) at the domain Healthcare.gov, or states could set up their own state-based exchanges (SBEs). While the Health Security Act envisioned the regional health alliances controlled by states as the default, the ACA saw the FFM as the default choice with states needing to opt in to creating an SBE.

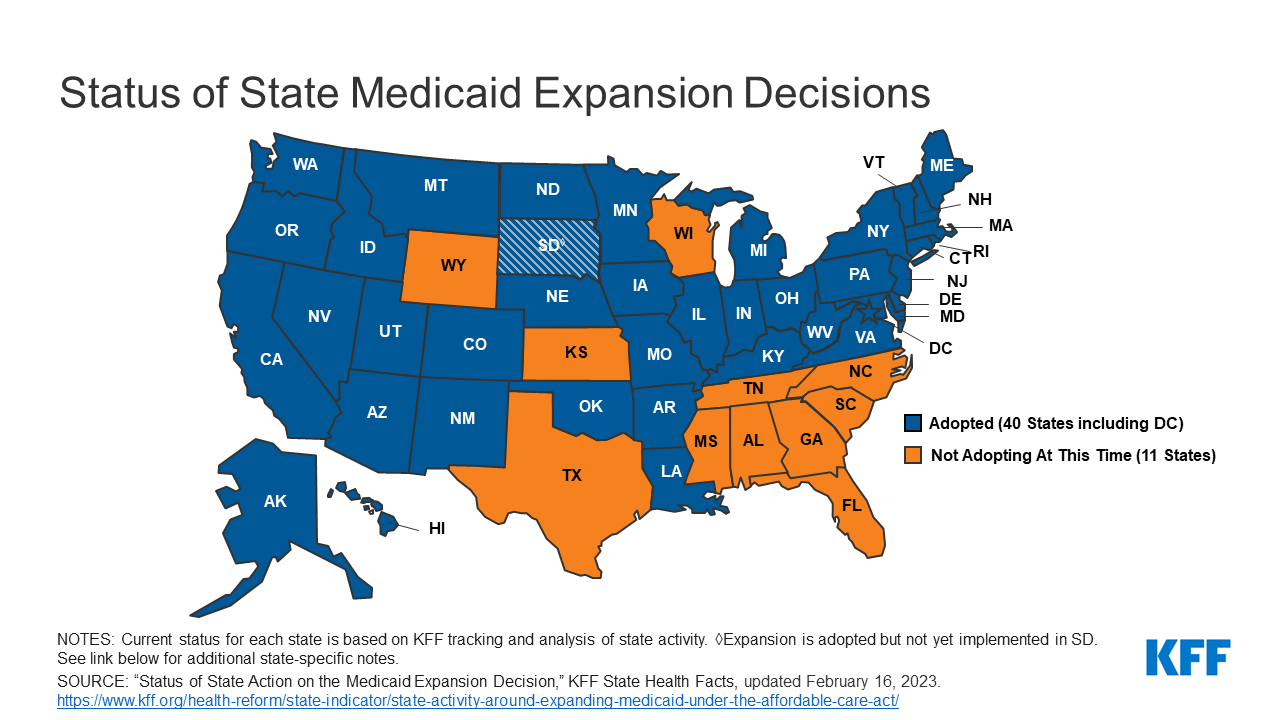
Another difference is that while the Health Security Act rolled Medicaid enrollees onto the regional health alliances with subsidies, the ACA chose to expand Medicaid for childless adults up to 138% of the poverty line. While the Health Security Act desired a common market for everyone not on Medicare, the ACA instead chose to use the FFM solely for those without some government plan or employer insurance. Medicaid Expansion was intended to be de facto required, but in 2012 the Supreme Court made it a voluntary opt-in program much like original Medicaid. As of today, 11 states have not expanded Medicaid, though states continue to expand.
In contrast to the Health Security Act’s new long term care benefit, the ACA included the CLASS Act, which was a voluntary federal long term care insurance program. However, this was repealed prior to launch because the voluntary nature of the plan would lead to adverse selection and it was considered inviable.
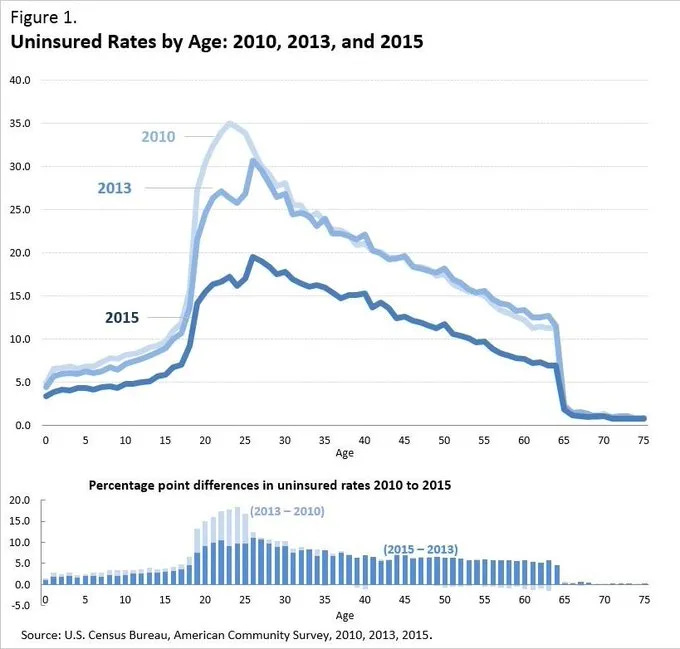
The ACA was passed in 2010 and the markets launched in 2014. Though it wasn’t enough to achieve universal coverage, it did substantially reduce the uninsured rate, particularly among young adults. Around 2 in 3 newly insured people were covered by the Medicaid Expansion, while 1 in 3 gained employer coverage or purchased it on the new marketplaces.
The Trump Administration and the failed ACA repeal effort

The GOP, and conservative policy thinkers, were never much of a fan of the ACA. Much like their response to the Health Security Act, they despised the potential adverse selection from guaranteed issue and the community rating. Some thought the income-based tax credits from the ACA over subsidized the poor and could lead to work disincentives as the benefit phased out. They thought tying the subsidies purely to income could lead to further health care inflation, and that the individual mandate was the wrong way to go about enforcing coverage. The Medicaid Expansion to them was another government hand out, and the employer mandate a simple tax on businesses that would harm smaller entities and make it harder to compete. But with President Obama in the White House even a GOP Congress, with a House takeover in 2010 and Senate in 2014, couldn’t prevent the ACA from being implemented. Then, in 2016, the GOP retake the White House with the election of Donald Trump. ACA repeal, a dream for years, was finally possible with a GOP trifecta.
Immediately upon taking office, President Trump and the GOP Congress undertake the effort to repeal and replace the ACA. An excellent in-depth comparison of the plans to the ACA was covered in Uwe Reinhardt’s book Priced Out. However, many organizations came out with their own summaries of the differences between the House repeal plan, the American Health Care Act (AHCA) and the Senate plan known as the Better Care Reconciliation Act (BCRA). Under both the AHCA and BCRA, the employer mandate was repealed as was the individual mandate. The AHCA replaced the individual mandate with a 30% surcharge for people that lacked continuous coverage, while the BCRA had no effective replacement. The AHCA relied on state waivers to establish essential health benefits with the default as repeal of it, while BCRA kept them with state waivers if states wanted to modify them. Pre-existing conditions protections remained for people that kept continuous coverage in the AHCA, but were left in place in the BCRA. The AHCA allowed for underwriting based on health status with a waiver, while the BCRA did not. Both the AHCA and BCRA increased the age band formula from the ACA’s plan of allowing the elderly to be charged 3 times the premiums of the young to 5 times the premiums of the young, but the AHCA allowed for a waiver to exceed this while the BCRA simply allowed states to choose a different formula. Both plans phased out the Medicaid expansion over time, and created path ways to block grant original Medicaid. Both plans expanded the limits on total contributions allowed in tax-free health savings accounts, and both plans created reinsurance and risk corridor programs for high expense enrollees. Finally, the AHCA replaced the income based refundable tax credit tied to the local cost of insurance for people between 100%-400% poverty with a flat age-based tax credit that phased out after $75,000. Americans under 30 would get a $2,000 credit while Americans over 60 would get a $4,000 credit. BCRA kept the ACA’s monthly paid income-based and geographic structure of the credits up to 350% poverty, but based the tax credits on a less generous plan than the ACA’s benchmark Silver plan. Both plans eventually eliminated CSR payments.
The Congressional Budget Office estimated that as many as 24 million people would lose their health coverage if the AHCA were passed with similar numbers from the BCRA. These plans would effectively reverse all of the progress from the ACA, though some conservative analysts disagreed with the analysis. Regardless, the AHCA tax credit structure would only reduce the cost of a premium somewhat. If you made just too much to get Medicaid, your premiums could skyrocket from nothing to $9,000 instantly. The full effect of the tax credit for the even the elderly would do little to make it more affordable, let alone the young.
While the BCRA kept the income-based and geographic tax credit structure of the ACA, albeit less generously, the AHCA was much closer to the original Heritage Foundation plan of flat tax credits. And the results showed. This plan would “get people closer to affordability,” but it would still lock out the poor to hold down the cost of premiums. And a return to medical underwriting if coverage wasn’t continuous meant that the sick could once again be discriminated against for their conditions, though in a more roundabout way. Allowing much greater state control and much weaker federal regulation of plans, though not a full return to the pre-ACA landscape, was an ideological step back towards something the Heritage Foundation would be comfortable with.
In the end, both the AHCA and BCRA collapsed, and the GOP lost the House of Representatives to the Democrats, preventing another attempt. The Tax Cuts and Jobs Act, or Trump tax cuts, set the individual mandate to $0, but no other major changes were made. As a consolation prize, President Trump removed CSR funds from the ACA market in an attempt to sabotage the marketplace, though states and insurance companies adapted to increase tax credits through what is called “Silverloading.” And to attempt to deregulate the market, President Trump loosened regulations on health care sharing ministries and association health plans, and allowed for short term health plans to be held all year. This effectively created a long term off-market series of plans that would allow for underwriting, though without any tax credits to support it.

Conclusion
Though the ACA, passed by a Democratic President with a Democratic Congress, shares refundable tax credits in common with the Heritage Foundation plan, it was ultimately much more similar to President Clinton’s Health Security Act of 1993 than the Heritage Foundation Plan. Though it did not attempt to merge the Medicaid, employer, and individual markets like the Health Security Act, it: created the FFM and SBEs instead of regional health alliances, used progressive income and geography tied refundable tax credits paid monthly for a progressive premium scheme, regulated insurance nationally and set up a standard package of benefits, set up expense benchmarks, and set up transfers between insurers to make them closer to administrators than fully private entities. The AHCA repeal plan offered by the GOP President and House, by contrast: used flat age based refundable tax credits like the Heritage Foundation plan, repeals the individual mandate, allowed for greater underwriting, eliminated the Medicaid Expansion and employer mandate, loosened the standard benefits package, and eliminated many of the insurance regulations in favor of state control.
In the end, the ACA bears little resemblance to the Heritage Foundation plan, but much more closely resembles the plan laid out 17 years earlier by President Clinton and the Democratic Congress of the early 1990s. The repeal efforts offered by the GOP are much closer to the conservative alternative offered in the 1990s and in the early George W. Bush Administration. The usage of tax credits is the beginning and end of their kinship. And any confusion of this fact will render you unable to access to concrete ideological differences in the two parties in how they approach health care policy in the United States.