

Safety Net Providers, Charity, and Debt: How America cares for the uninsured and underinsured


Introduction
America’s uninsured population, around 26 million people in total, lack comprehensive health coverage. For children, just under 2% are uninsured. These people are left paying out of pocket for their care, and without many of the benefits the rest of us enjoy. As of 2019, the Kaiser Family Foundation found about 9 in 10 people with some legal status were eligible for Medicaid, subsidies for Obamacare, had an employer insurance offer, or had high enough income to afford a plan without subsidies. But thanks to the confusion inherent in America’s health care system, many remain uninsured.

Rather than leave the uninsured without any assistance, a hodgepodge of programs have been developed over the years to grant them access to basic health care. This includes government funding for Safety Net Hospitals, health centers, federal mandates to stabilize patients regardless of ability to pay, mandated charity care at non-profits hospitals, as well as care at free clinics and programs to reach the underserved parts of the country. While these programs cannot be a substitute for comprehensive health care, they do represent a significant effort to care for this population. In what follows, I will review these programs.
Safety Net Hospitals and Disproportionate Share Hospital Payments
Safety Net Hospitals are the first key tool used to care for the uninsured. These are the 25% of hospitals that provide the most inpatient care for the uninsured and people with Medicaid, about 1,000 hospitals in total. They provide key health care and other health services to the uninsured. These hospitals can be public or private, for profit or non-profit, but they cannot turn away patients by ability to pay. In return for accepting any patients, Safety Net Hospitals receive additional transfers like Disproportionate Share Hospital (DSH) Payments, increased Medicare payments, and more.
DSH payments are Medicaid payments made to hospitals that provide uncompensated care to a disproportionate share of poor and uninsured patients. In Fiscal Year 2020, these payments totaled $19.5 billion, $8.2 billion from states and $11.3 billion from the federal government. States began to make these payments in 1981 when Medicaid payments were delinked from Medicare rates in order to compensate for the harm to safety net hospitals from this change. States were slow to begin these payments, so the federal government allowed for donations, required states submit plans to make these payments, and more. DSH payments are also capped in total and per hospital by the Federal Financial Participation (FFP) amount.
FQHCs, CHCs, SBHCs, and more
The safety net isn’t limited to hospitals, the government also funds Federally Qualified Health Centers (FQHCs) under Section 330 of the Public Health Services Act as well as increases in Medicare and Medicaid reimbursement. FQHCs must provide for underserved populations, offer a sliding scale fee based on income for people up to 200% the poverty line, and provide preventative care, dental care, mental health and aid for substance abuse, transportation for care, and hospital and specialty care. They also must have a quality assurance program and have a governing board of directors. Not all organizations that meet FQHC standards receive FQHC funding. These “look alikes” can still receive enhanced Medicare and Medicaid funding.
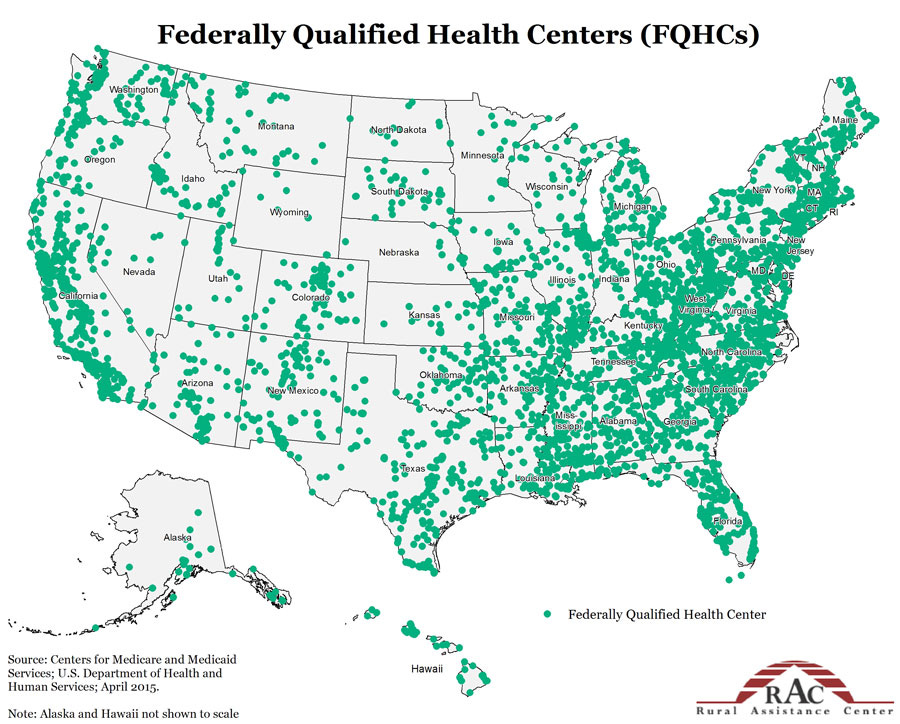
FQHCs are the overarching group, but it encompassed several types of health centers: Community Health Centers (CHCs), Migrant Health Centers, Health Care for the Homeless Health Centers, Public Housing Primary Care Centers, or centers operated by Native American tribes. These programs were consolidated in the 1990s and funding increased with the passage of the Affordable Care Act.
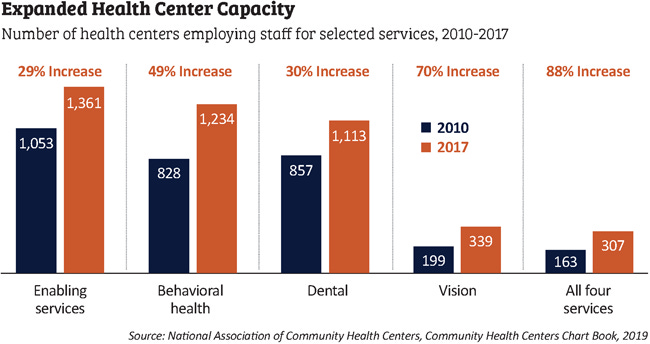
CHCs, which began in 1965, serve over 30 million Americans in 13,000 communities across the country. These beneficiaries include 1 in 3 people living in poverty, 1 in 5 people in rural areas, 1 in 6 Medicaid enrollees, 1 in 8 people of color, and 1 in 9 children. With the passage of the Affordable Care Act, an additional $11 billion was allocated over 5 years to double capacity over time. As a result, services have increased across the board in the last few years.
Migrant Health Centers, created in 1962, serve 800,000 migrant farm workers and their families.
The Health Care for the Homeless Program began in 1987 and now serves more than 1.4 million people experiencing homelessness each year.
Public Housing Primary Care Centers provide care for 856,000 public housing beneficiaries and 4.4 million people total across 108 sites. These enrollees disproportionately suffer from chronic diseases, diabetes, asthma, obesity, and more. These centers offer care on-site for needy Americans.
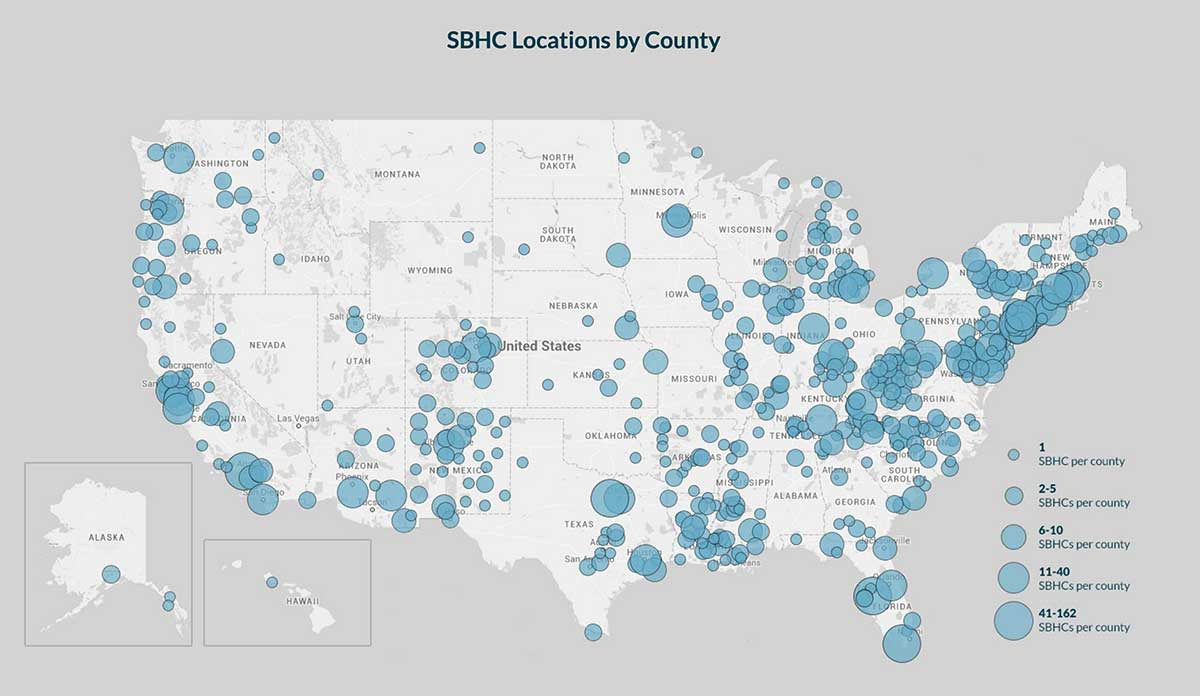
School Based Health Centers provide basic primary care services for 2 million children in 2,000 locations across the country. About half also provide mental health services, and 10% provide basic dental care. These centers get a mix of federal and state funding and other revenue sources.
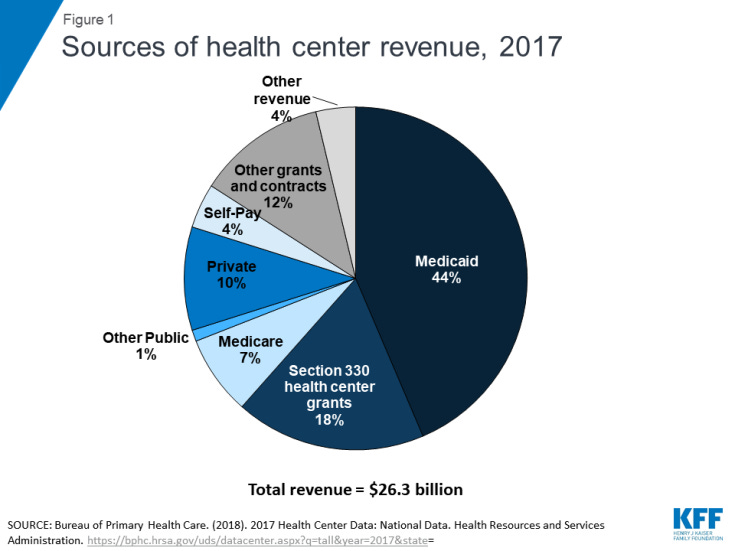
Health Center funding comes from a variety of sources. Nearly half of revenue comes from Medicaid, with a small amount of funding from Medicare, about a fifth of total funding comes from Section 330 of the Public Health Services Act, with the remainder coming from private spending, out of pocket spending, and grants.
Rural Health Clinics provide primary care in rural areas through a different funding mechanism than FQHCs, but still provide an important service.
To fill staffing holes, the government created the National Health Services Corps in 1972. Participating providers serve 21 million Americans across 10,000 CHCs via 20,000 funded clinicians. This partnership offers to forgive up to $50,000 in student loan debt for two years of full-time service and $25,000 for part-time service for clinicians.
EMTALA

Even with the development of Medicaid and Medicare in 1965, 15% of Americans remained uninsured prior to the Affordable Care Act. With the creation of safety net hospitals and providers, there was a worry that non-government institutions would discharge patients without an ability to pay to public hospitals prior to ensuring the patients were stabilized. In 1985, Congress passed the Emergency Medical Treatment and Labor Act (EMTALA). This law applied when patients came to the emergency room, the aim being that a patient with an acute condition severe enough that a lack of treatment could seriously endanger their or an unborn child’s health. If a patient requires treatment or an examination at an emergency department, the treatment cannot be delayed to ask about insurance. The treatment is given, and a transfer will occur (with no ability to reject the patient) if the department the patient showed up to lacks the ability to treat the patient.
About 95% of emergency physicians provide uncompensated care each week, and 55% of an emergency physician’s time is spent on uncompensated care. They even treat two-thirds of all acute care among the uninsured even though they only comprise 4% of physicians. If a provider fails to offer EMTALA related treatment, they can be fined ~$60,000-~$120,000 per case, can be excluded from Medicare and other public insurance, and can be a target of a civil suit. Naturally, DSH payments and FQHCs were created or expanded around the same time this law was passed, so they could be seen as working in tandem.
Charity Care, Free Clinics, and RAM
Of course, not all health insurance in the United States is funded by the government, and neither is care for the uninsured. The US has a large market for charity care, free clinics, and non-profits like Remote Area Medical (RAM).
As a part of the Affordable Care Act, the IRS requires non-profit hospitals to offer charity care, but the specifics are not laid out. Some hospitals may only offer aid to the uninsured, others will offer some aid to the underinsured, or may get what funding they can via Medicaid or other programs first. This process is imperfect to say the least. It can take weeks, can be denied, many bills contain billing errors, and more. And some hospitals make it a business model to attempt to collect payment, any payment, even among patients that qualify for charity care. The American health care system is a complex web with hidden pitfalls, and there is no shortage of them for the uninsured.
Aside from charity care, there are also 355 registered free clinics in the US that serve about 650,000 uninsured Americans. These clinics are non-profits with a collection of revenue from donations and government funding that exist to offer free services to the uninsured. Modern free clinics started in the late 1960s as an effort to provide drug treatments and other basic services to the needy. Many were started in the inner city, but they also spread to rural areas. They were founded by non-profits, medical students, and even the Black Panthers as an effort to treat patients otherwise shut out from the health care system. Though they don’t offer the full range of service other settings can, they may be the only type of care the homeless or undocumented immigrants can receive.
Permanent clinics aren’t the only charity solution though. In 1985, RAM was founded to help offer periodic free care in remote rural settings where there was a dire need for care. Volunteers go annually to treat basic medical, dental, vision, and other needs. People will line up for hours for the chance to have teeth pulled, or just to get a cleaning for free.

Medical Debt, Charity Forgiveness, and GoFundMe
If all else fails and the patient still gets treatment, they may be saddled with some form of medical debt. According to the Kaiser Family Foundation, 23 million Americans (9%) have some medical debt. About 11 million Americans (3.3%) owe more than $2,000 in medical debt and 3 million (~1%) owe more than $10,000. In total, there was $195 billion in medical debt in 2019. By comparison, only about 3% of people in the United Kingdom, Sweden, France, Germany, and Japan face medical bills large enough to threaten their economic security.
People with medical debt are more likely to be young or just below the Medicare age, disabled, poor, a minority, or in poor health. This problem likely stems from the fact that 32% of households could not afford a $2,000 bill, and half of households could not afford a $6,000 bill. With deductibles and out of pocket maximums being much higher than this for many people with private insurance, this outcome is nearly inevitable. And for the uninsured, a lack of coverage leaves them unprotected. While both Medicaid and COBRA can be retroactive for a couple months for those eligible, there is still a significant gap in the health care system leading the rising problem of medical debt.
To address this need, some non-profits like RIP Medical Debt are stepping in. When medical debt goes into collections, it will affect your credit after the first few hundred dollars. But hospitals often sell the medical debt for pennies on the dollar to outside agencies to own the debt and collect on it for a profit. RIP Medical Debt turns this business model on its head by accepting donations, using the money to purchase medical debt, and forgiving the balance for far less the cot than the value of the debt. So far, they have purchased $6.7 billion in unpaid debt and forgiven the debt for 3.6 million people at a cost of $1 for every $100 of debt. A small amount relative to the total amount of medical debt, but life changing for the people affected.
Finally, some people have taken matters into their own hands and turned to online websites like GoFundMe to ask others for help online. Webpages even exist to make yourself more “marketable” and increase your donations.
As you can see, it’s not that the United States does nothing for the uninsured. Tens of billions of dollars are spent to cover uncompensated care, 13,000 or more health centers provide care for 30 million Americans, free clinics are spread throughout the country, charity care has been set up, and clinics are placed in school and sent to remote regions. But it still pales in comparison to true comprehensive health coverage and access to care. In fact, the Center for American Progress estimated that even closing the Medicaid gap would save 7,000 Americans, result in 48,640 fewer evictions, and prevent $2 billion in medical debt each year. Let alone what the benefits may be to covering every American. Having a safety net is crucial. Declining to give every American comprehensive coverage, even through an omission of administrative burdens, costs us debt, displacement, and lives every year.